
Third Edition - Preventing Spread of Coronavirus Disease 2019 (COVID-19) Guideline for Airlines
Preventing Spread of Coronavirus Disease 2019 (COVID-19)
Guideline for Airlines
Third Edition
In order to prevent and control the spread of COVID-19 via aircraft, and act in accordance with the principle of “targeted and detailed prevention and control measures”, the multi-level, categorized and differentiated management of outbreak containment for air transport is implemented. Meanwhile, in order to further refine personal prevention and protection requirements for crew members, maintenance personnel and cleaning staff, improve requirements on environment hygiene, disinfection and maintenance for aircraft, and introduce prevention and control measures for special transport missions (chartered flights etc.) to/from high-risk infection countries (regions) and handling procedures for transfer passengers in Beijing from high-risk infection countries (regions), the Preventing Spread of Coronavirus Disease 2019 (COVID-19) Guideline for Airlines – 3rd Edition is developed on the basis of amendment to the second edition.
1. Standards for Grade Level of Flight Infection Risks and Principles of Disease Prevention and Control
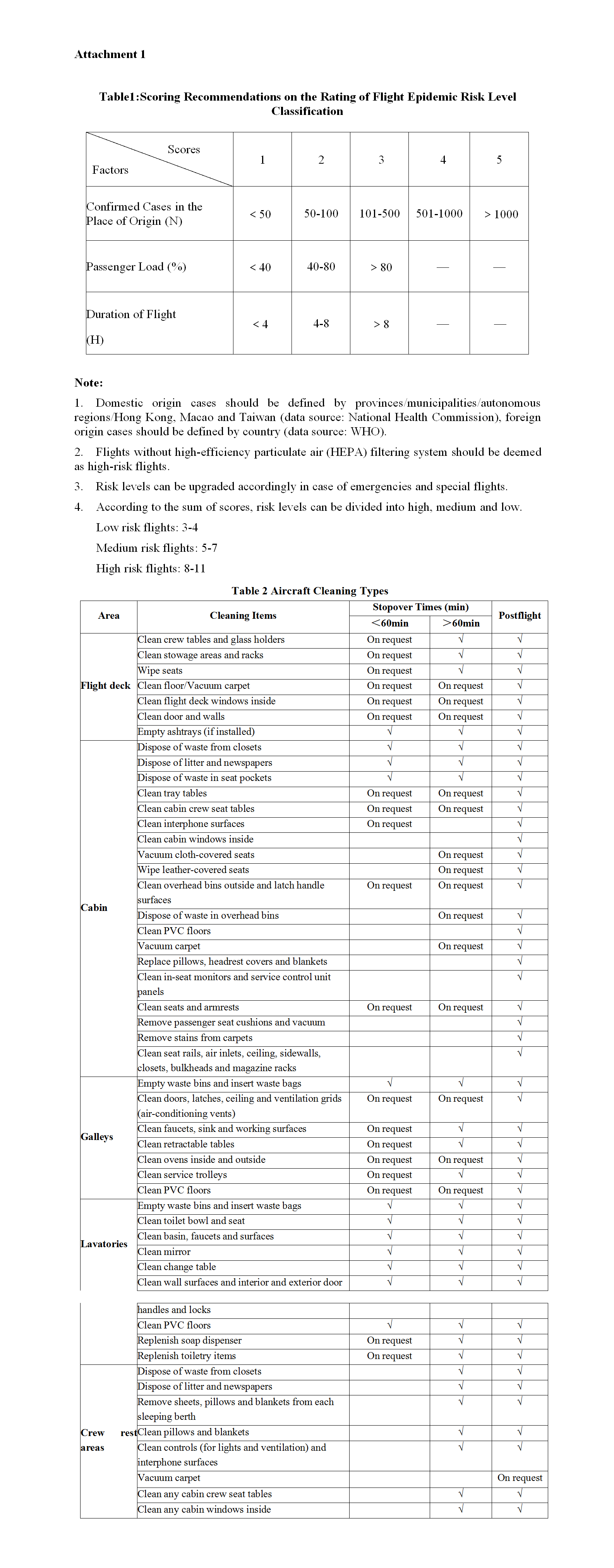
Transport flights should be categorized into the three levels, namely high-risk flights, medium-risk flights and low-risk flights, and differentiated prevention and control measures should be applied after a comprehensive evaluation of the outbreak at the place of origins of the flights (both international and domestic), whether the aircraft is equipped with high efficiency particulate air (HEPA) filters and other indicators such as load factors, flight time and mission of the flights. Risk levels should be subject to dynamic adjustment in line with the development of the outbreak. Standards for the grade level of risks can be found in Attachment 1.
2. Temperature Screening
According to the risk levels of different flights, passengers’ body temperature should be measured at different phases of flights.2.1 Low Risk FlightsNon-contact infrared thermometer equipment (calibrated) should be used to measure the body temperature of passengers and the symptoms should be observed as required. One should timely report and respond in case of ill passengers found with symptoms including fever (≥37.3℃), fatigue or dry cough, etc., then cooperate with local health authorities in the handover of the ill passengers.2.2 Medium and High Risk FlightsThe measurement of passengers’ body temperature should be carried out before boarding and in-flight based on flight segments and flight distance.
2.2.1 Pre-enplaning
Non-contact infrared thermometer equipment (calibrated) should be used to measure the body temperature of passengers and the symptoms should be observed before boarding, and timely report and response should be made in case of suspected passengers found with symptoms including fever (≥37.3℃), fatigue or dry cough, then support should be given to local health authorities in handover of the suspected passengers.
2.2.2 In-flight
For high-risk long-haul (>4h) flights, in-flight measurement of body temperature during operation should be taken. In case of ill passengers found with symptoms including fever (≥
37.3 ℃), fatigue or cough, the occurrence should be dealt with in compliance with the handling measures of in-flight emergencies of this Guideline and the crew should timely communicate with destination airports, and then hand over the ill passengers after landing in cooperation with local health authorities.
3. Infection Control Measures for Crew Members
3.1 Personal Protective Equipment (PPE)
Given the risk level of flights, different prevention and protection measures should be taken:
3.1.1 Low-risk flights: wearing protection of disposable medical masks (up to YY/T0969- 2013 or equivalent standards) or facial masks of a higher standard.
3.1.2 Medium-risk flights: wearing protection of surgical masks (up to YY0469-2011 or equivalent standard) or masks of a higher standard.
3.1.3 High-risk flights: flight crew should wear surgical masks or masks of a higher standard and goggles, and change facial masks every 4 hours in general (or anytime considered necessary, similarly hereinafter). Cabin crew should wear N95 particular matter protection facial masks (up to GB2626-2006 or equivalent standard) or medical protection masks (up to GB19083-2010 or equivalent standard), goggles, and disposable rubber gloves, and change facial masks every 4 hours.
Crew members should reduce entering the cockpit and using separate toilets. Intercom system is recommended for communication among crew members to avoid close contact.
3.1.4 Discarded masks should be placed in a distinct bin, sprayed or sprinkled till fully soaked with chlorine disinfectant (500mg/L-1000mg/L) before post-flight cleaning, and packed in a tightly knotted plastic bag for centralized disposal.
3.2 Considerations
The mask should be close to the face, covering the nose and mouth completely, leaving no space. During in-flight service and when removing the mask, the crew should not touch the outside of the mask with their hands to avoid contaminating their hands. The facial masks should be changed with new ones as soon as they are damp or contaminated and hands should be cleaned with sanitizer both before and after the replacement.
The crew can use alcohol-based disinfection wipes to clean and disinfect their hands. When the crew is not sure whether their hands are clean, avoid touching the nose, mouth and eyes with their hands. When sneezing or coughing, one should try to lower the head or turn away from passengers and crew members nearby, and cover the mouth and nose with tissue or flexed elbow. After touching or disposing wastes, hands should be cleaned with soap or hand sanitizer under running water followed by hand disinfection.
4. Advice for In-flight Service
4.1 Low and Medium Risk Flights
Food-preparing procedures should be simplified, pre-packaged food should be provided, and cold meal and ice should be canceled to reduce exposure risks and avoid cross-infection. Lavatory should be cleaned every 2 hours (or anytime considered necessary, similarly hereinafter) during flight, and once finished, hands should be timely cleaned and disinfected.4.2 High Risk FlightsCabin crew should avoid close contact with passengers and only provide necessary in-flight service. It is recommended to hand over pre-packaged food and bottled water before or during boarding. Unless it is required specially, catering service should not be provided onboard.
Flight attendants should be assigned to provide service for certain areas, and flight attendants designated should provide basic service for the crew members when needed. Efforts should be made to arrange passengers to sit in separation. Lavatory should be cleaned at least every hour during flight, and once finished, hands should be timely cleaned and disinfected.
The last three rows of seats should be reserved as quarantine areas when handling possible in- flight emergencies.
5. Routine Cleaning and Preventative Disinfection of Aircraft
5.1 PPE for Cleaning Crew
5.1.1 Low and medium risk flights
One should wear surgical masks or masks of a higher standard, uniform, disposable snood cap, disposable rubber gloves, work shoes (as necessary), waterproof apron and protections against chemicals such as disinfectants.
5.1.2 High risk flights
One should wear N95 particular matter protection masks or masks of a higher standard, disposable mop cap, goggles, disposable protective suits, medical rubber gloves and disposable shoe covers.
5.2 Routine Cleaning
Wet process cleaning for aircraft should be applied during a stopover to avoid the onward spread of infections matters, and a thorough cleaning upon the completion of the flight should be carried out. For detailed cleaning methods, please refer to Attachment 2. If conditions are limited, lavatory and gallery should be cleaned in priority.
5.3 Preventative Disinfection
Preventative disinfection should be carried out after the aircraft is cleaned.
5.3.1 Frequency
Preventative disinfection should be done on a regular basis, at least once a week, for low risk flights; and every time after flight for medium and high risk flights. An assessment on the effect of post-flight disinfection may be carried out for high risk flights if conditions allow.
5.3.2 Rules of operation
● Separate rags and mops should be used for aisle, lavatory and gallery, and mark them with different colors to avoid cross-contamination. Different personnel should be tasked with each of the aforementioned areas when conditions allow.
● During disinfection, surfaces should be rubbed using rags soaked with disinfectant, after a period of time for reaction, the regular cleaning process should be finished, to avoid erosive effect on cabin component due to long time exposure to the disinfectant.
● Disinfectant should be sprayed to cabin floor from the front to the back, then key areas should be disinfected. Once cabin disinfection is finished, disinfectant should be sprayed to cabin floor again from the back to the front.
● Disinfection of key areas should proceed in the following order:
Aisle: Ceiling, overhead bins, reading lights, air outlets, sidewall panels, windows, seats (tray tables, armrests, passenger control units, decorative panels), cabinets/lockers, bulkheads, magazine racks, cabin attendant seats.
Lavatory: The disinfection in lavatory should be progressed from contaminated to clean areas, as follow: toilet bowls, waste bins, basins, lavatory sidewall, ceiling, door assembly (door surfaces, doorknobs, ashtrays, if installed, and latches)
Gallery: Ceiling, ovens, water boilers, coffee makers, galley facilities, lockers/drawers, waste bins.
5.3.3 Disinfectants
Aircraft cleaning and disinfectant products that have been approved for airworthiness should be used (refer to http://www.fccc.org.cn/webs/xhg/list.aspx?classid=0202 for products list, similarly hereinafter) to avoid corrosive aircraft components. Given the characteristics of current epidemic and knowledge, the following is recommended for wiping disinfection, their concentration should refer to products use instruction:
It is recommended to use compound quaternary ammonium salt, double-chain quaternary ammonium salt, hydrogen peroxide and chlorine-containing disinfectant. For hydrogen peroxide, concentration should be no higher than 3% and reaction time be 20 minutes; effective concentration of chlorine should be within the range of 250mg/L-500mg/L, and reaction time be 10 minutes.
6. Aircraft Maintenance
6.1 PPE of Maintenance Crew
The following prevention and protection measures should apply when replacing a high efficiency particulate air (HEPA) filter:
6.1.1 One should wear a particulate matter protection mask or medical protection mask, snood cap or disposable mop cap, goggles, disposable protective suits, medical rubber gloves and disposable shoe covers.
6.1.2 The mask should be close to the face. Do not touch and adjust the mask, goggles and protective cap during operation.
6.1.3 Avoid hitting, dropping, or shaking the HEPA filter. Do not use compressed air to clean the filter. Used HEPA should be placed in a special plastic bag, disinfected with chlorine disinfectant and sealed.
6.1.4 After the task is completed, the maintenance staff disinfects the hands first, then removes the protective equipment in order, and thendisinfects the hands again.
6.1.5 Discarded disposable protections should be placed in dedicated plastic bags and sealed for centralized disposal.
6.2 Routine Maintenance
6.2.1 During ground operation and maintenance, aircraft auxiliary power unit (APU) should be used for ventilation, and avoid using bridge load air source. After arrival, doors of cabin and cargo compartment should be opened for ventilation before performing maintenance work and extend the natural ventilation time.
6.2.2 HEPA filters should be replaced in accordance with standards specified in the manufacturer’s manual, and the replacing process should be in strict compliance with the prevention and protection requirements of the Aircraft Maintenance Manual, and refer to the personal prevention and protection program for aircraft maintenance personnel.
7. Handling of In-flight Medical Emergencies
7.1 Infection Control Measuresfor Crew Members
Upon contacting ill passengers (having symptoms such as fever, fatigue or dry cough), or treating body fluids (such as respiratory secretions, vomit, blood, diarrhea) or contaminated objects and surfaces, cabin attendants should wear personal protective equipment (PPE) found in the Universal Precaution Kit (UPK).
7.1.1 Gloves: Cabin attendants should wear double-layered disposable rubber or butyronitrile gloves. If there are more than 2 ill passengers on board, hands should be disinfected before contacting other passengers.
7.1.2 Masks: Cabin attendants should wear medical protection masks. Touching or adjusting masks is prohibited during emergency handling.
7.1.3 Goggles: Reusable goggles should be promptly sterilized and dried every time after use. Goggles with a anti-fogging film should avoid being wiped with disinfectant. Instead, it is recommended to be washed with water then exposed to close-range direct ultraviolet lighting for over 30 minutes
7.1.4 Protective clothing: When contacting ill passengers, suspected or confirmed patients, cabin attendants should wear goggles and disposable protective clothing (replace by the protective apron in the UPK as an interim emergency measure).
7.2 On-board Emergency Quarantine Measures
The ill traveler (passenger or crewmember) should be quarantined on-board by the following methods:
7.2.1 The last 3 seat rows of the cabin should be designated for relative emergency quarantine. If possible, the ill traveler should be seated in the right window seat, by which the breath exhaled could be exited the cabin directly to the largest extent.
7.2.2 The right rear lavatory should be specifically designated for quarantine purpose. It is recommended to assign specific crew members to provide necessary in-flight service for quarantine areas, and the crew members should minimize close contacts (within 2 meters) with other crew members and unnecessary contacts.
7.3 Aircraft Concurrent Disinfection
The cabin contaminated with body fluids/substances (such as respiratory secretions, vomit, blood, diarrhea,) should be disinfected timely according to the procedures in Emergency Medical Equipment Installation and Training for Large Transport Aircraft (AC-121-102R1 issued by CAAC).
7.3.1 Wearing personal protections(PPE);
7.3.2 Preparing disinfectant: One should take one surface disinfection tablet and put it into 250-500ml clean water to make a 1:500-1000 disinfectant;
7.3.3 Covering the respiratory secretions, blood, vomit, diarrhea and other contaminants evenly with absorbent disinfectant for 3~5 min to enable them solidified;
7.3.4 Shoveling the coagulated contaminants with portable pickup shovels into biohazard wastes bags;
7.3.5 Sterilizing contaminated area with pre-prepared disinfectant, making sure disinfectant stays at the contaminated surface for 3-5 minutes, then washing the area with clean water for three times before drying the area with towels. Put those towels and other used disinfection materials into biohazard wastes bags;
7.3.6 Disinfecting hands before removing protections by the following order: taking off protective suits (aprons), gloves, applying skin disinfection wipe for hand disinfection; then taking off goggles, facial masks, and at last applying skin disinfection wipe to clean hands and other parts of the body that may have been exposed to contaminants.
7.3.7 Placing all used protections and contaminated items inside a biohazard wastes bag; closing the bag, filling a label with “Biohazard Waste”, then tagging it on the seal.
7.3.8 Keeping the tied bio hazard waste bag in a proper place temporarily to prevent it from missing, being damaged or contaminating meals on board.
7.3.9 Informing ground departments at the destination to prepare for takeover.
7.4 Aircraft Terminal Disinfection
After carriage of ill passengers, terminal disinfection should be conducted.
7.4.1 After all people get off the aircraft, close cabin doors, adjust the air conditioning to high-volume to complete all-round air exchange.
7.4.2 Once the air exchange is finished, first the sitting area of ill passengers and lavatory should be disinfected, then clean other areas in accordance with the post-flight cleaning requirements.
7.4.3 After cleaning, one should proceed with terminal disinfection by following the general principle of thorough disinfection from out ring-to-center, top-down and encompassing-approach.
7.5 Aircraft Cargo Hold Disinfection
If animal corpses or suspicious contaminants of a contagious nature are found in the cargo hold, post-flight terminal disinfection should be performed . The disinfection procedures are as follows:
7.5.1 When animal corpses or suspicious contaminants of a contagious nature are found in the cargo hold, the contaminated area in which the animal corpses or the contaminants were should be disinfected and cleaned as the first step, followed by a thorough disinfection of the remaining areas of cargo hold.
7.5.2 The method of spray disinfection and enclosed disinfection should be used. Disinfection should be performed from the upwind to the downwind direction and from top to bottom. Before disinfecting the inside area of the cargo hold, the personnel in charge of disinfection should spray around the door, close the door, enter into the cargo hold, and spray on the floor in front of the cleaner while moving forward till the whole floor is sprayed before disinfecting other areas of the cargo hold. The personnel should disinfect the ceiling of the cargo hold by spraying disinfectant from left to right and vice versa, and then spray the cargo hold wall from top to bottom. While disinfecting the ceiling and the wall, the amount of disinfectant sprayed should not exceed the amount of the liquid that can be absorbed (the maximum amount of disinfectant the surface can absorb). Upon completion, the cargo hold floor should be disinfected again by spraying while moving backward. After returning to the ground along the ladder, the ladder should be sprayed.
7.6 Disinfectant
Aircraft cleaning and disinfection products should be approved for their airworthiness. During terminal disinfection, the passenger cabin should be wiped while the cargo hold should be sprayed with disinfectant. The liquid concentration should be in line with what’s specified in the product application instructions.
It is recommended to use hydrogen peroxide or chlorine-containing disinfectant. The concentration of hydrogen peroxide should be the same as that used in preventive disinfection, and the effective concentration of chlorine should be 1000mg/L, for 30 minutes. The air conditioner should be turned off during the disinfection operation, and the passenger cabin or cargo hold should be fully ventilated after disinfection.
8 Quarantine Management for Crew Members
According to the COVID-19 Prevention and Control Program of the National Health Commission (the fifth edition, or the latest edition if updated), the quarantine program of crew members should be based on the following guidelines.
8.1 Crew Members Quarantine Management
8.1.1 If any crew member shows symptoms such as fever, fatigue or dry cough, and has a history of epidemiology (such as a history of living, traveling and having contacts with locals in high-risk countries/regions), he/she should be dealt with in accordance with the requirements in the COVID-19 Prevention and Control Program. Other crew members who have been on the same flight with him/her within the 2 days preceding the appearance of the above symptoms should be instantly put under centralized quarantine, and where conditions do not allow, they can be put under house quarantine and medical observation.
8.1.2 If any crew member shows symptoms such as fever, fatigue or dry cough during the duty, he/she should cease performing his/her duties immediately. It is recommended to put him/her under quarantine in the last 3 rows of seats to avoid close contact with other crew members. If he/she has a history of epidemiology, after the flight has landed and the passengers and other crew members have deplaned, a special vehicle should be sent, carrying him/her to a designated medical facility for examination. Other crew members should be quarantined as per 8.1.1.
8.1.3 Where any passenger onboard shows symptoms such as fever, fatigue or dry cough, and/or has a history of epidemiology, he/she should be transferred in a special vehicle after the flight has landed and other passengers and crew members have deplaned. The flight attendants designated to provide onboard services for the symptomatic passenger and otherattendants in the same cabin section should be picked up by a special vehicle to a location for centralized quarantine, and where conditions do not allow, they can be under house quarantine and medical observation. Other crew members do not need to be quarantined for the time being, but close attention should be paid to their health conditions.
8.1.4 Where an airline has been informed by the local disease control or quarantine department that a flight of the airlines carried confirmed, suspected or asymptomatic patients, it should notify the crew members flying the flight segment concerned for centralized quarantine, where conditions do not allow, they can be under house quarantine and medical observation.
8.1.5 Where crew members fly charter flights and other special flights (such as those used for emergency transportation of materials and medical teams) to/from high-risk areas in China, they generally do not need to be under medical quarantine and observation after returning, provided that they can make good pre-return preparations by strictly observing the following requirements.
● No crew members should be allowed to disembark the aircraft (ground handlers should be requested to do external inspections, refueling, etc.);
● No ground personnel should be allowed to embark the aircraft;
● The doors should be closed immediately for the return trip upon completion of the transport of assisting medical personnel and materials, without cleaning, water refilling or waste disposal at the destination airport;
● Aircraft maintenance. If there is no aircraft malfunction after landing, the crew members or in-flight maintenance personnel may issue a release from within the aircraft without the need for making a short stop for maintenance; an external inspection can be completed by qualified local personnel from outside the aircraft, and under condition other than the aforementioned, operators should carry out remote training and provide remote guidance to local personnel. If there are malfunctions in the aircraft after landing and a release cannot be issued based on the Minimum Equipment List (MEL), the malfunctions must be addressed before the flight operation can continue; where a release can be issued based on the Minimum Equipment List (MEL) but a maintenance (item M) procedure has to be performed, crew members should conduct a joint evaluation with the maintenance department, and under the premises of ensuring safety, remote guidance, simplified maintenance and equivalent measures can be taken to allow the aircraft to fly back to the base; where a release can be issued based on the Minimum Equipment List (MEL) but a crew operation (item O) procedure has to be performed, the crew can, if the conditions allow, continue the flight after completing the item O procedure;
● Terminal disinfection of the aircraft should be performed after its return to the home base;
● Before the aircraft lands, the flight dispatcher should inform the crew members once again to make preparation for the return trip by following the above five bullet points.
8.1.6 For those crew members who carried out special transportation missions (charter flights) to/from countries (regions) with high incidence of COVID-19, they should be under medical observation as per what’s stipulated in Article 9 of this guideline.
8.2 Quarantine Period
The medical observation period refers to 14 days after the last contact of the quarantined crew members with confirmed, asymptomatic, suspected or suspicious passengers or other crew members. During this period, if the suspected or suspicious patients have been clearedby the disease control department, the quarantine and medical observation of the above- mentioned crew member can be removed.
8.3 Quarantine Measures
8.3.1 Crew members under medical observation should report their body temperatures and health conditions to the relevant department of the airlines every morning and evening.
8.3.2 Crew members under centralized or house quarantine should stay in a relatively separate space which should be regularly cleaned and disinfected, and minimize their contact with other people living together.
8.3.3 Crew members under observation must not go out during the observation period. If they have to go out, they shall report to the relevant department of the airlines, wear a surgical mask and avoid crowded places.
8.3.4 The airlines concerned should keep a record of the health conditions of the crew members under medical observation, as well as the number of times they went out.
8.3.5 Once a crew member under observation shows any symptoms during medical observation (such as fever, chills, dry cough, cough, expectoration, nasal congestion, runny nose, sore throat, headache, fatigue, muscle soreness, breathing difficulties, dyspnea, chest tightness, conjunctival hyperemia, nausea, vomiting, diarrhea, abdominal pain etc.), the airlines should report to the local public health department immediately and send the crew member to the designated medical care facility for diagnosis and treatment.
8.3.6 After the medical observation period, the crew member under observation should be released from medical observation if showing no signs of symptoms.
9. Infection Control Measures for Special Transport Missions (Charter Flights) to/from Countries (Regions) with High Incidence of Epidemic Infection
9.1 Assessment of Passengers’ Fitness to Fly
Passengers should be assessed for their fitness to fly before enplaning, mainly to assess whether they are physically suitable for this specific flight. Health assessment should be done by the health department.
Before carrying passengers, relevant department of the airlines should check the health conditions of the passengers by screening. Confirmed or suspected cases or those who can pose potential health risks shall not be transported on the same plane carrying healthy passengers, and in general, close contacts shall not be transported on the same plane carrying healthy passengers either.
Passengers are required to wear a surgical mask or facial mask with better filtering capabilities throughout the journey, and in case of N95 masks, the ones without breathing valves should be used.
9.2 Temperature Screening
9.2.1 Pre-boarding
Non-contact infrared thermometer equipment (calibrated) should be used to examine the body temperatures of the pre-boarding passengers taking a charter flight and observe any
potential symptoms. If any suspicious passenger with symptoms such as fever ( ≥ 37.3 ℃), fatigue or dry cough is found, he/she should be verified immediately using a mercurythermometer. If confirmed as a passenger with fever, he/she shall be under accompanying medical staff’s care and shall not be transported by air for the time being.
9.2.2 In-flight
For long-haul flight exceeding 4 hours, the cabin crew and healthcare workers should examine the body temperatures for passengers during the flight. If any suspicious passenger with symptoms such as fever ( ≥or d3r7y.3co℃ug),h fiastigfouuend, the crew should notify the healthcare workers. If necessary, the crew should take some basic measures based on the guidance for the handling of in-flight emergencies, issue a timely notification to the destination airport, and provide cooperation in the transfer of passengers after landing.
9.3 Cabin Area Division
In order to avoid cross-infection, the cabin area can be divided into clean area, buffer zone, passenger sitting area, area for close contacts (if any) and quarantine area. The division should be made based on the following principles (and can be adjusted taking into account different aircraft types):
9.3.1 Clean area: it is recommended that the front half of the cabin for both the first and business class be designated as a clean area for the exclusive use by crew members. No one wearing protective clothing shall be allowed to enter the clean area. The boarding gate connecting the clean area should be reserved for the exclusive use by crew members.
9.3.2 Buffer zone: it is recommended that the rear half of the cabin for both the first class and business class be designated as a buffer zone available for use by crew members to wear and take off protective clothing.
9.3.3 Passenger sitting area: it is the sitting area for healthy passengers. Passengers should be seated with at least one empty seat between each other.
9.3.4 Area for close contacts (if any): close contacts, if required to be transported, should be seated with at least one empty seat between each other, and should be at least two rows of seats away from the passenger sitting area.
9.3.5 Quarantine area for ill traveler: the last three rows of seats should be designated as the emergency quarantine area (observation area).
9.3.6 Each area should be clearly labeled, and it is recommended that a disposable curtain be used for the physical separation of each area.
9.3.7 Lavatories: the lavatory in the first-class cabin is to be used exclusively by crew members and needs to be thoroughly disinfected after each use. The lavatory on the rear right side of the cabin is for the exclusive use by the close contacts or the quarantined cases, and the surface area should be disinfected every hour during the flight, with the hands cleaned and disinfected right after the completion of disinfection.
9.3.8 Cabin crew members should manage each cabin area separately, and prohibit passengers from moving across different areas. Passengers sitting in different cabin areas should enplane and deplane in separate groups.
9.4 Infection Control Measures for Crew Members
9.4.1 PPE
Ÿ Personal Protection equipment for cabin crew members: medical protective masks, double-layer disposable medical rubber gloves, goggles, disposable medical caps, disposable protective clothing, and double-layer disposable shoe covers. It’s recommended that cabin crew wear disposable diapers and avoid using lavatory unless in special circumstances to reduce the risk of infection.
Ÿ Personal Protection equipment for flight crew members: surgical masks or facial masks with better filtering capabilities, and goggles. It is recommended to change the facial masks every 4 hours. Disposable protective clothing and/or disposable shoe covers can also be worn if so required by a specific task.
9.4.2 PPE wearing/taking-off procedure
Wear: disinfect hands - wear hat - wear facial mask - wear the first layer of shoe cover - wear the first layer of gloves - wear protective clothing - wear protective glasses - wear the second layer of shoes cover - wear the second layer of gloves;
Take off: disinfect hands - take off protective goggles - take off the second layer of shoes cover - take off protective clothing (the second layer of gloves) - disinfect hands - take off facial mask - take off hat - take off the first layer of shoes cover - take off the first layer of gloves - disinfect hands.
9.4.3 Dinning considerations
Cabin crew members should be divided into different groups while having simple meals in different hours of the day. To reduce the risk of exposure, others should refrain from walking around.
9.5 In-flight Service Considerations
9.5.1 Flight attendants in different cabin areas shall be managed separately and provide separate in-flight services. The flight crew working area, passenger sitting area, area for close contacts and quarantine area for ill traveler on an aircraft shall be served by different flight attendants. In principle, flight attendants are not allowed to leave the area they serve, and they should avoid close contact with passengers or other flight attendants.
9.5.2 Only pre-packaged food and bottled drinking water will be provided, which are placed in the back pocket of the front seat before boarding. Except for special needs, catering service will no longer be provided during the flight.
9.6 Handling of In-flight Emergencies
9.6.1 If there are any suspicious passengers on board showing such symptoms as fever, fatigue or dry cough, an arrangement shall be made to sit them in the quarantine area.
9.6.2 Once the cabin is found to have been contaminated by blood, secretions, excreta, vomit and other liquids, it shall be disinfected instantly following the specific procedures in Article 7 - Handling of In-flight Medical Emergencies, paragraph 3, sub-paragraph 3 - ongoing aircraft disinfection.
9.6.3 For other considerations, please refer to the relevant description in the Handling of In- flight Medical Emergencies.
9.7 Procedure for Crew Members Deplaning after Operation
9.7.1 After landing, the aircraft shall park at a remote stand (no bridge docking allowed), and a special passage shall be set aside for crew members, in order to avoid mixed flow with passengers. The flight crew shall deplane after the cabin crew members have deplaned, and they shall be picked up separately by a special vehicle.
9.7.2 Cabin crew members shall take off their protective equipment at the door and change their facial masks before deplaning.
9.7.3 Flight crew members are prohibited from opening the cockpit door unless cabin crew members have deplaned. Protective equipment should be changed in the cleaning area.
9.7.4 All the discarded protective equipment of crew members shall be placed in special yellow medical waste bags and be centrally disposed of as medical waste.9.8 Aircraft DisinfectionTerminal disinfection shall be performed after landing, by referring to the specific procedures as detailed in Article 7 - Handling of In-flight Medical Emergencies, paragraph 4, subparagraph 4 - terminal disinfection of aircraft passenger cabin.
All wastes in the cabin shall be centrally disposed of as medical waste.9.9 Quarantine Management for CrewmembersAll crew members shall be put under a centralized quarantine and medical observation for 14 days. During the period of centralized observation, they shall monitor their physical conditions on a daily basis, and are not allowed to go out except for the urgent need to fly a charter flight.
During the period of centralized quarantine and medical observation, if a flight crew member is required to fly yet another charter flight, the quarantine period shall be recalculated.
10. Procedures for Handling of Passengers (with Normal Body Temperature) from High-risk Countries Transferring at Domestic Airports
Any passengers with normal body temperature from high-risk countries (regions) transferring in Beijing should be handled in accordance with the following procedures, which can be used as a reference by other airports in China:
10.1 The airport shall coordinate with local customs to set up a special waiting area, coordinate with the public security department and health quarantine or disease control department to quarantine the passengers in question, and provide them with basic daily necessities such as food. For passengers staying overnight, the airport shall make timely contact with the local government which shall make arrangements to place the passengers under quarantine at a designated place. After the passengers’ departure, terminal disinfection shall be performed in the quarantine waiting area.
10.2 Accompanying airport staff should wear facial masks, gloves, goggles or face screens.
10.3 The airport shall adopt such measures as simplifying boarding formalities, setting up a quarantine passage, and assigning a designated person to monitor the passengers, in a bid to prevent cross-infection at the airport, and shall promptly provide the airlines concerned and destination airport with information on the passengers, enabling them to make preparations for the proper handling of the incoming passengers.
10.4 The passengers in question shall enplane before others and deplane after others. They shall be arranged by the airline to sit by the window in the last three rows, and use exclusively the bathroom on the rear right side of the cabin. The airlines will provide pre- packaged food and water in advance, and will not provide them with any direct on-board services.
10.5 Passengers with abnormal body temperatures and passengers who will not transfer after landing shall be handed over to the relevant local departments for follow-up action.
11. Methods of Psychological Self-Regulation for Front-line Personnel of Airlines
The front-line personnel can chose the following methods to protect themselves from psychological crisis and maintain a good mental health state.
11.1 Having a Good Understanding of Own Emotional Experience
It is normal to have certain negative emotions during the epidemic, and these unusual emotions can in turn serve as a reminder to protect ourselves in a more timely and effective manner. Even if we find that we have some emotional experiences we don’t familiar with, we needn’t to be stressful. It is normal for us to have these psychological changes. If we allow these reactions to occur and accept what is happening, rather than deny and reject them, positive changes will naturally ensue.
Where our negative emotions cannot be relieved through self-regulation, resulting in extreme fear and anxiety, even affecting our sleep and diet, it’s recommended to seek professional help.
11.2 Acquiring the Epidemic Information with a Proper Attitude
The huge amount of information about the epidemic will leave us with a strong sense of anxiety and helplessness. We should avoid being influenced by emotionally charged information. We’d better to seek information from formal media and official websites, and never fall victim to certain rumors. Also, we should develop a proper plan on when to get information online, and in particular try to avoid exposure to influx of information at the time when we feel most fragile (such as right before bedtime). And last, we should avoid the vicarious trauma caused by information overload. We need to leave enough time for ourselves to listen our inner voice and be aware of our emotional changes. That can help us to turn panic into appropriate personal protection.
11.3 Friendly and Mutual Social Support
Social connection can calm us down. Communicating with others is the most effective way to relief our stress. On the one hand, through frequent communication with family and friends by telephone and the Internet, we can encourage each other, share our feelings and reinforce mutual psychological support; on the other hand, by making contact with colleagues in similar situations, we can lend our ears to each other and renew our connections, in a bid to building a psychological anti-epidemic alliance.
11.4 Maintaining a Stable and Healthy Lifestyle
Maintaining a regular working and resting schedule and having a sense of self-control are the good panacea for anxiety and panic. Although our ranges of activities are restricted, we still can take a positive look at life. We should, to the greatest extent possible, maintain our regular schedule and follow our usual daily routine, allowing us to return to our normal life. In addition, we should develop good living and hygiene habits, keep a healthy diet, have enough sleep, and never try to ease our tension through the use of tobacco and alcohol.
12. Proper Use of Personal Protective Equipment
In order to provide guidance to front-line staff in civil aviation on how to correctly wear facial masks, hats, gloves, goggles and other protective equipment, our office made a video, downloadable from the website ams.caac.gov.cn under Prevention and Control of Public Health Emergency.
This is an un-official translation for reference.
Should there be any discrepancy in interpretation, the original Chinese version shall prevail.
更多动态
外国航空运输企业航空安全保卫规定
为进一步科学规范外国航空运输企业航空安全保卫工作,保证旅客、机组、航空器和公众的安全,民航局公安局研究制定了《 外国航空运输企业航空安全保卫规定》。
- Seventh Edition-Preventing the Spread of Coronavirus Disease 2019 (COVID-19) Guideline for Airlines
- Seventh Edition-Preventing Spread of Coronavirus Disease 2019 (COVID-19) Guideline for Airports
- 关于新冠疫情常态化防控期间规范国际定期客运航班计划管理的通知
- 民航局关于调整国际客运航班熔断措施的通知
- 关于进一步落实来华航班乘客实施远端防控措施有关工作的通知
- 关于切实做好来华航班乘客凭新冠病毒核酸检测阴性证明登机有关工作的通知
- 民航局、海关总署、外交部关于来华航班乘客凭新冠病毒核酸检测阴性证明登机的公告(附英文参考译文)
- 关于目的地为北京的国际航班从指定第一入境点入境的公告(第3号)(附英文参考译文)
- 关于精准做好国际航空货运机组人员疫情防控工作的通知(附英文参考译文)
资料下载
-
2020-03-10
